Infectious Microorganisms Do Not Care About Your Existing Policies
The transmission of infections is once again in the forefront of worldwide concerns. The current Ebola virus outbreak which started in Africa has killed many people and the future of this epidemic is unknown.
When studying infectious disease transmission and prevention, the hospital as a building is a virtual guinea pig. The high rates of patient deaths due to healthcare-associated infections (HAIs) indicate that this guinea pig is very sick indeed. Why is the hospital physical environment a place where infections flourish?
Hospitals are shelters and enclosures for:
• A human population very susceptible to infections — patients;
• The most aggressive pathogens — multi-drug resistant organisms such as Methicillin Resistant Staph Aureus (MRSA) and opportunistic pathogens such as Clostridium Difficile;
• Difficult-to-access and -clean “nooks and crannies” in the walls and ceilings where medical gas lines, electrical wires, and HVAC ducts reside — interstitial spaces where pathogens can hide and reproduce.
In addition to these components, hospital administrative and organizational dynamics make understanding and preventing HAIs very difficult. Without a full understanding of the current situation, verifying the benefits of change is impossible. What are some of the components of this impetus to open communication? The facility managers and engineers who run the hospital have very different professional training and educational backgrounds from the doctors and nurses who care for patients. Each group has years of education on subjects that do not intersect, creating silos of knowledge and unspoken hierarchies that can make communication extremely difficult. In addition to knowledge silos there are:
• Clinical staff who are usually rushed and often tired, making cutting corners a likelihood;
• Housekeeping workers who are among the lowest paid, yet who have the essential job of cleaning rooms between patient admissions;
• Administrative and clinical staff who regulations onerous;
• Layers upon layers of internal and external guidelines;
• Recently, government financial penalties for open disclosure of HAIs.
Even though challenging existing regulations and guidelines seems like an almost insurmountable obstacle when communication and teamwork is strained, statistics on the incidence of patient deaths due to hospitalization show that it is imperative to take new approaches to improve patient safety. The non-disruptive route of following existing policies without researching their efficacy is no longer acceptable. Infectious disease transmission and HAIs need to be interrupted!
The current situation in hospitals
There is scientific evidence that many infectious microorganisms are transmitted through the air on fomite carriers of tiny droplets, particles, skin flakes, or dust. Despite this evidence, airborne transmission is currently minimized in hospital infection control strategies, which are dominated by interruption of direct transmission routes such as unwashed hands. While rules on hand hygiene are essential, they are not sufficient.
Why is airborne transmission not adequately addressed? There are many reasons, most of which are beyond the scope of this article. One, however, will be addressed here. Many researchers use the term “airborne” to describe only “obligate airborne organisms,” or pathogens that ONLY travel through the air and initiate infection in the lungs. This definition excludes pathogens that are spread by direct contact, but can also be spread over long distances through the air on fomites and instigate infection through the lungs, nasopharynx, gastrointestinal tract, or breaks in the skin.
A definition of airborne transmission that looks beyond a microbiologist’s view of the organism would include all air transmission of the pathogen to the patient becoming infected. Most pathogens that can be spread by direct contact can also be carried through the air on fomites. This expanded definition of airborne transmission emphasizes the criticality of hospital indoor air management as an infection control step.
Focusing on IAQ
IAQ guidelines are historically based on comfort measures — primarily odor and smoke clearance. At some point in time, probably with the advent of tuberculosis, airborne infection control became more obviously a problem in hospitals, so air pressurization and turbulence control were introduced to direct “dirty” air away from clean areas. To date, however, there are few controlled studies proving that these air-handling strategies improve patient outcome.
Review of the research reveals that the current IAQ recommendations for air handling in patient rooms are still largely based on comfort studies (ASHRAE Transactions, 2012) with little scientific data to correlate a particular number of room air changes with improved patient outcome. Historically, IAQ studies on controlling occupant comfort and odor control use smoke and other carbon based molecules as the test material. Infectious particles found in hospitals, however, are made up of lipids, polysaccharides, and proteins. The movement and infectivity of bacterial, viral, and fungal organisms vary with the RH of the air, whereas carbon based molecules do not respond in the same way. Because of these differences, comfort and odor studies are not an accurate basis for preventing airborne transmission of pathogens.
Regulations currently state that increased ventilation rates yield increased patient safety; however, infection control studies show that this is not necessarily the case. Excessive turbulent air movement can actually decrease patient safety as well as cause unneeded energy expenditure. Controlling air physical characteristics such as RH and turbulence to support the health of patients is underutilized as an infection control precaution.
BUT: Biology knows no silos, and it doesn’t care about regulations! What indoor air parameters can improve the health of the occupants of a hospital?
“Moisture content may, indeed, be the most important environmental factor influencing the survival of airborne microbes.” — Dimmick, Naval Biological laboratory, Univ. CA, Berkeley
RH, the measure of the percentage of water vapor held by the air, is not identified as an indoor air contaminant nor as a significant factor in preventing health problems. This is an oversight, as low indoor air RH is harmful to patients in several ways. Dry air harms our body’s physiological barriers that fight infections, and it enhances survival and transmission of many pathogenic organisms.
The successful transmission of airborne infectious diseases in hospitals is dependent upon several factors: the number of people introducing infectious droplets, the vulnerability of patients, and the length of patient exposure to the organism. The length of patient exposure is determined by the rate at which infectious aerosols settle out of the air, and by the survival of pathogens in aerosols during transmission. Maintaining the relative humidity of hospital indoor air between 40% and 60% can significantly decrease HAIs by the following mechanisms.
1) The patient physiological barriers in passages from the nose to the depths of the lungs are most functional at room RH of 40% to 60%. Mucus-lined passages prevent pathogens from invading into deeper body tissues by continually washing particles away. This critical defense mechanism is impaired by dry air, enabling harmful organisms to reach deep lung tissue and the blood stream.
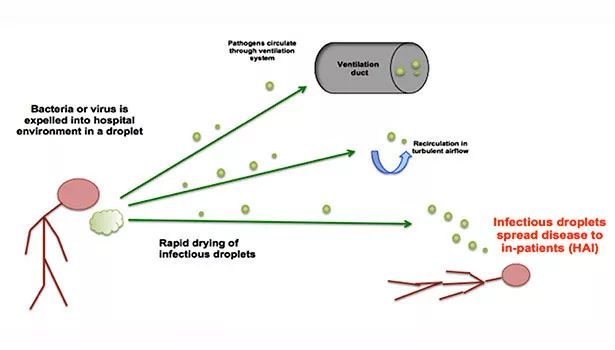
2) When indoor air is dry, the size of droplets carrying infectious particles shrink quickly, enabling the pathogen to be carried on air currents over great distances. When the RH is maintained from 40% to 60%, these infectious droplets settle within 4 ft to 6 ft of their source (a person sneezing, toilet flushing). In 1934, Wells observed the evaporation of droplets in dry air and concluded that large droplets strike the floor, while smaller droplets evaporate to create tiny droplet nuclei with significantly extended residence time in the air.
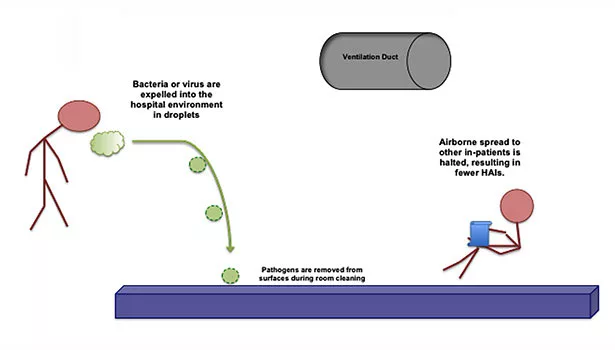
Humans shed roughly a billion skin cells daily with each square centimeter of skin having a concentration between 100 to 10,000,000 bacteria. Results from studies demonstrate that many airborne bacterial organisms originate from human skin, hair, nostrils, and the mouth through shedding and are subsequently circulated in droplet aerosols. When the RH is 40% to 60%, these infectious droplets settle quickly onto the floor and horizontal surfaces, re-suspension is prevented, and effective room cleaning with surface disinfectants eradicates the pathogens, thereby decreasing the length of patient exposure.
3) While suspended during airborne transmission in dry air, infectious microorganisms are often temporarily in “travel mode,” behaving as if they are dead and non-infectious if collected at this time. But these same microbes can be highly infectious when inhaled.
4) Studies show that many viruses and pathogenic bacteria have decreased viability in RH between 40% and 70%. Reducing pathogen survival decreases direct transmission of infections as well as related allergic illnesses such as asthma. Many respiratory viruses such as influenza, severe acute respiratory syndrome-associated coronavirus (SARS), respiratory syncytial virus, Para influenza, measles, rubella, varicella zoster, and respiratory adenoviruses and rhinoviruses survive the longest at low RH of 15% to 30% and the most briefly at 40% to 60% RH.
Clearly, monitoring and controlling RH to limit the airborne spread of HAIs is essential to patient safety and hospital cost containment. Unfortunately, healthcare facility guidelines are moving toward lowering the allowed minimum RH in operating rooms. This could further promote airborne transmission of infectious diseases such as MRSA, Acinetobacter spp. and Pseudomonas spp., Clostridium difficile, and Vancomycin Resistant Enterococci (VRE). In addition, there are no regulations for monitoring relative humidity in patient rooms and clinical spaces.
Decrease Room Air Changes (RAC)
There is strong evidence associating building air movement via ventilation with increased spread of measles, tuberculosis, chickenpox, influenza, smallpox, and SARS. In addition, there is insufficient data to support increased RACs and the prevention of infectious disease spread via the airborne route in hospitals, schools, offices, and homes.
Turbulent airflow also plays an important role in airborne transmission. While turbulent airflow can dilute airborne contaminants, it can also cause cross-infection to other patients. Pathogens emitted in droplets via coughing, sneezing, talking, and breathing or the direct shedding of skin-associated pathogens initially settle on surfaces, only to become re-suspended in dry, turbulent airflow. Genetic pieces of bacteria found on human skin have been recovered in indoor floor dust, suggesting that re-suspension of this dust may carry human-associated bacteria. These findings highlight the importance of fully understanding the influence of both RAC and turbulence in forced and naturally ventilated systems.
In summary
Indoor air movement and RH are important building components that can affect patient healing through both maintenance of the patient’s physiological barriers and through the movement of many pathogens, whether or not these pathogens are currently classified as “obligate airborne organisms.”
Looking for a reprint of this article?
From high-res PDFs to custom plaques, order your copy today!








