Accepting Airborne Transmission of SARS-COV-2: Our Greatest Fear and Greatest Opportunity
The time has come to embrace the A-word.
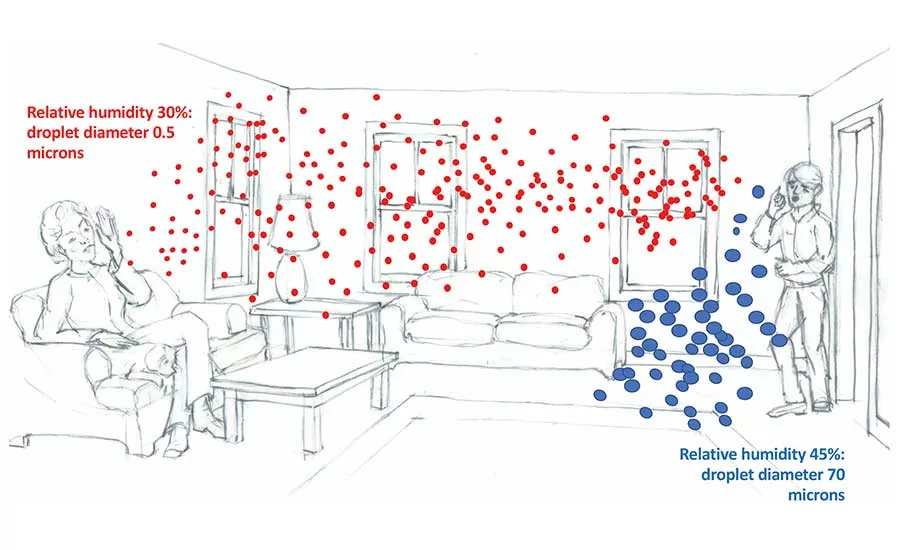
Large exhaled droplets evaporate to different degrees, and in low relative humidity buildings become tiny droplet nuclei that are truly airborne. An RH of 30% is depicted on the left, and 45% RH is shown on the right. Drawing courtesy of Alan Guazzoni.
As we move into summer, many unanswered questions about the COVID-19 pandemic remain. Who gets sick and why? What are the routes of transmission, and how do we stay safe? What activities can we return to and when?
This is not the first and will not be the last pandemic caused by a highly infectious virus. Nevertheless, people are scared and want control or at least predictability. Unfortunately, the primary certainty we have right now is that we have few familiar benchmarks.
One of the most active debates is whether or not the SARS-CoV-2 virus is transmitted over significant distances through the air. In summary, it looks like it is! There is enough evidence of airborne transmission that, out of prudence, we need to address this vector in our management of COVID-19.
There is compelling historical precedence for accepting airborne transmission. For example, when the Black Death decimated the European population during the 14th century, up to 60% of people living in London died between the autumn of 1348 to the spring of 1349. The transmission of the causative Yersinia pestis bacterium was blamed on flea-carrying rats. In 2018, however, genetic analysis of 25 skeletons unearthed in London told a different story. Researchers in England concluded that the bacterium must have been transmitted through the air in order for it to have spread through the population so quickly. In other words, the pneumonic vector was much more important than considered at the time. If people had realized this, they could have taken intentional steps to decrease airborne contagion rather than focusing almost entirely on controlling rodents.
We do not want to miss any opportunity to decrease the spread of COVID-19. The same genetic analysis techniques used to examine the London corpses have broadened our understanding of the transmission vectors of pathogens. When the respiratory tract is the primary organ in which replication or colonization occurs, there is some amount of long-distance aerosol transmission.
By acknowledging the airborne route, we open up the most effective toolbox available to us, that of managing the indoor environment. Thankfully, we have an abundance of tools to do this. The ASHRAE Epidemic Task Force has created an excellent website to guide building managers in the operation of HVAC systems during occupied and unoccupied times.
For example, we know that humidifying the indoor air to between 40%-60% relative humidity decreases the number of infectious particles in the air and simultaneously bolsters our respiratory immune system — a two-for-one benefit. Fresh-air ventilation helps dilute indoor contaminants. Infectious viral particle counts indoors can be lowered by proper filtration, UV light irradiation, and other air-disinfection strategies.
In order to have the motivation to use ASHRAE guidance, we have to understand that indoor airborne transmission is a likely route through which SARS-CoV-2 spreads. While this sounds scary and difficult to control, ignoring it is even worse. If we do not acknowledge it and continue to focus solely on short range and contact transmission with social distancing, face masks, and hand and surface hygiene, we will have suboptimal results and become even more divided over the correct way to move forward.
Looking for a reprint of this article?
From high-res PDFs to custom plaques, order your copy today!




