Air Distribution in Critical Facilities

FIGURE 1: Operating rooms (ORs) are rooms that meet the requirements of restricted areas that are designated and equipped for performing surgical or other invasive procedures and have the environmental controls for an OR as indicated in ANSI/ASHRAE/ASHE Standard 170.
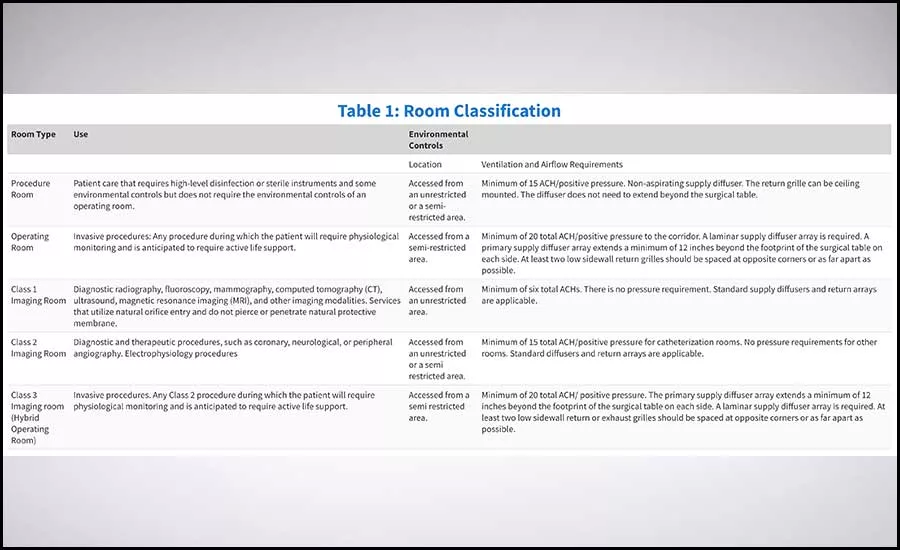
TABLE 1: Room classifications by location and environmental control type.

Critical facilities may include, but aren’t limited to, hospitals, health care centers, nursing homes, schools, police stations, and fire and emergency response installations as well as installations that produce, use, or store hazardous materials or hazardous waste. We could go a step further and define them as facilities that are critical to the health and welfare of the population and those that are especially important following a natural disaster or another disruptive occurrence. Critical facilities are vital because they provide essential services and protect lives and property. A loss of one of these critical facilities would result in severe economic and catastrophic impact.
Another layer of critical facilities are mission critical facilities. These facilities are broadly defined as containing operation that, if interrupted, will negatively impact business activities ranging from loss of revenue to jeopardizing legal conformity to, in extreme cases, loss of life. Some of the facilities that meet these criteria are hospitals, laboratories, data centers, public safety centers, and military installations. There is no uniform definition of mission critical, but, essentially, these facilities must maintain continuous operation. This means redundant cooling systems and power must be available at varying degrees of reliability. For power reliability, the National Fire Protection Association (NFPA) 70: National Electric Code, Facility Guidelines Institute (FGI) Guidelines, ASHRAE standards, and presidential directives offers some guidelines, but the design for reliability depends on the owners' and design engineers’ interpretation of which systems are mission critical and which are not.
This article will focus on air distribution within health care applications and define why it is important to get the design right for these mission critical facilities.
The design of airflow systems in health care environments is governed by strict safety and environmental standards. One of the most important design parameters is effective airflow design (EAD). The adherence to EAD serves to meet ventilation and air distribution requirements and limits the flow of airborne contaminants that can cause severe illness and loss of life.
Mechanical ventilation systems are the primary mechanism for controlling airborne infections in hospital environments. The goals of ventilation systems are to replace contaminated air with clean air, minimize the mixing of dirty and clean air, and regulate ambient temperature and humidity. One of the most important requirements of airflow systems in critical spaces is to maintain the pressure relationships that are required by the ANSI/ASHRAE/ASHE 170 Guidelines in all modes of operation. These systems, whether they are in hospital or ambulatory care facilities, must have fully ducted systems in order to maintain the required pressure relationships.
The airflow design and pressurization in these critical spaces must take into account filter loading during air-handling unit operation, heating season low-airflow operation, and cooling season high-airflow operation. There are several critical spaces within health care settings that require key attention to detail for airflow design. They are as follows: operating rooms, hybrid operating rooms, airborne infection isolation (AII) rooms, and protection environment (PE) rooms. There are other rooms that can be considered, such as emergency department (ED) rooms, trauma, neonatal intensive care unit (NICU) rooms, etc., but they will not be discussed as a part of this article.
Guidelines and Standards
All of the aforementioned critical rooms require a unique and strategic approach to the air distribution and temperature control. The current standards are guided by past and ongoing industry research by teams of health care professionals who work to evolve the guidelines to meet the required health care safety guidelines. The primary objective of air distribution is to ensure the cleanest air is supplied first to patients, then the rest of the space, then it’s filtered and mixed with outside air before it’s returned to the space and the process is repeated again and again. Most jurisdictions have adopted some version of the FGI recommendations, the latest being the 2018 version. The FGI guideline is supported by ANSI/ASHRAE/ASHE Standard 170, “Ventilation of Healthcare Facilities.” The international Code Council (ICC) formed an ad hoc committee on health care to ensure that multiple standards interpretations are not driving up the cost for construction and operation of these health care facilities.
Thermal comfort is extremely important for critical spaces in health care settings and is governed by ASHRAE Standard 55, “Thermal Environmental Conditions for Human Occupancy.” The airflow conditions in critical spaces are dependent on the air quality, ventilation rates, room temperature, and humidity. ANSI/ASHRAE/ASHE Standard 170 also has stipulations regarding design temperatures and maximum and minimum humidity levels. While the scope of Standard 170 includes occupancy comfort, it should not be assumed that meeting prescriptive design minimums will ensure compliance with ASHRAE Standard 55. Important design steps must be taken by the design team to ensure the spaces in the health care setting are treated appropriately to maintain the thermal comfort of the staff, visitors, and patients.
Operating, Procedure, and Imaging Rooms
The definition of operating rooms was redefined in the 2018 FGI Guidelines and has migrated from the prior definition of Class A, B, and C. The operating room or imaging room classification is dependent on the level of invasiveness, the type of sedation used to conduct the procedure, the number of staff expected, and the equipment needed to support the procedure. The room classification then determines the air distribution requirement of the space. The three critical spaces for design for these types of spaces are as follows:
- Procedure rooms (formerly Class A);
- Operating rooms (formerly Class B & C); and
- Imaging rooms (Class 1, 2 and 3).
Procedure Rooms
Procedure rooms are defined as rooms “designated for the performance of patient care that requires high-level disinfected or sterile instruments and some environmental controls but is not required to be performed with the environmental controls of an OR.”
The room is intended for procedures in which the body cavity or protective surface of the body may be penetrated but which do not meet the definition of “invasive.” The airflow requirement per ANSI/ASHRAE/ASHE Standard 170, Table 7.1, is a minimum of 15 air changes per hour (ACH). The room must be positive pressure with respect to the adjacent connecting corridor to the doors. A Group E, non-aspirating diffuser should be used in these rooms. The return grille can be in the ceiling, and there is no need to meet the full operating room specification as it relates to the laminar diffuser field and low returns. Diffusers do not need to extend beyond the surgical table.
Operating Rooms
Operating rooms (OR) are rooms that meet the requirements of restricted areas that are designated and equipped for performing surgical or other invasive procedures and have the environmental controls for an OR as indicated in ANSI/ASHRAE/ASHE Standard 170. An aseptic field is required for all procedures performed in an OR. The airflow requirement per ANSI/ASHRAE/ASHE Standard 170, Table 7.1, is a minimum of 20 ACH. Primary non-aspirating, Group E supply diffuser arrays extend a minimum of 12 inches beyond the footprint of the surgical table on each side. No more than 30% of the primary diffuser area should be used for non-diffuser applications. This means booms and light fixtures must not take up more than 30% of the primary diffuser array. The average velocity for the primary diffusers should be between 25-35 cfm per square foot. The room is required to have two low sidewall exhaust or return grilles, ideally placed on opposite corners of the room at a maximum of 8 inches above the floor.
ANSI/ASHRAE/ASHE Standard 170 allows OR setback for periods when the room is out of use; this means the room can reduce the ACH during unoccupied periods. It’s very important to ensure the pressure relationship is maintained during all modes of operation. The code requires a design relative humidity between 20%-60% for OR spaces; this sometimes cannot be achieved without introducing humidification in the winter and allowing dehumidification in the summer.
The face velocity for the primary diffuser should not exceed 35 fpm. The reason for this requirement is to control the rate of skin particle erosion off surgical team members. This will also minimize the overcooling of the patient to prevent hypothermic complications, uncomfortable drafts, and entrainment of contaminated air in the surgical zone.
Both ORs and procedure rooms are required to have positive pressurization with respect to the adjacent corridor the doors open to. The requirement is to maintain a positive pressure of 0.01 inch of water column. A good engineering practice is to allow 20% less return airflow than supply. The testing and balancing (TAB) contractor will ultimately determine the appropriate differential airflow to meet the required pressure requirement. In order to ensure the rooms are in compliance with the pressure requirements listed in ANSI/ASHRAE/ASHE Standard 170, it is a best practice to install a visual pressure indicator at the entrance to the rooms.
Imaging Rooms
Imaging rooms host imaging services. Depending on what takes place within the imaging room, the room may be used for diagnostic, therapeutic, or invasive procedures and, as such, should be designed to the same standards as those required for the procedures that take place in non-imaging settings. Table 1 describes the classification of imaging rooms and the types of procedures that are done in each type.
Class 1 imaging rooms shall have a minimum of six total ACH. There is no pressure requirement for these spaces, and they require standard supply diffuser and return grilles.
Class 2 imaging rooms shall have a minimum of 15 total ACH. Positive pressure is required for catheterization rooms. There are no pressure requirements for other imaging procedures for class 2 rooms, and these spaces require standard supply diffuser and return grilles.
This is a hybrid operating room, and, therefore, the room airflow requirements are similar to those of an OR. These rooms shall have a minimum of 20 total ACH. These rooms are required to be positive pressure with respect to adjacent corridors. Primary non-aspirating, Group E supply arrays extend a minimum of 12 inches beyond the footprint of the surgical table on each side. A laminar supply diffuser array is required. At least two low sidewall return or exhaust grilles should be spaced at opposite corners or as far apart as possible.
AII Room Air Distribution
AII rooms are very specialized rooms in hospital settings because they are used to control the spread of airborne infectious diseases. These rooms are designed to deliver a negative pressure differential to the surrounding areas to ensure that airflow is inwards to these rooms and not outwards. The rooms are designed to isolate a patient who is suspected of, or has been diagnosed with, an airborne infectious disease. The negative-pressure isolation room is therefore designed to help prevent the spread of a disease from an infected patient to others in the hospital.
ANSI/ASHRAE/ASHE Standard 170 requires a minimum of 12 air changes of supply airflow per hour and must maintain a minimum 0.01-inch-wc negative pressure differential to the adjacent corridor whether an anteroom is utilized or not. When an anteroom is provided, airflow should be from the corridor into the anteroom and from the anteroom into the patient isolation room. To maintain the required pressure differential, the exhaust air quantity must always be higher than the supply airflow. Typically, a minimum airflow difference of 20% is usually adequate to maintain pressure differential in a well-sealed room. The final differential airflow will need to be determined by the testing and balancing contractor. In order to ensure these rooms are operating per design ANSI/ASHRAE/ASHE Standard 170, permanently installed visual devices or mechanisms should be implemented to constantly monitor the air pressure differential (when occupied by patients with suspected airborne infectious disease).
ANSI/ASHRAE/ASHE Standard 170 recommends that supply air diffusers for AII rooms be located in the ceiling above the patient bed with the return air grille located in the ceiling near the door. The supply diffuser shall be a non-aspirating, laminar-flow device and should be designed to limit the air velocity at the patient bed to reduce the possibility of patient discomfort.
Protective Environment (PE) Rooms
These specialized rooms, which are used to protect patients who have compromised immune systems, are designed to offer a positive pressure differential to the surrounding areas to ensure airflow is inwards to these rooms and not outwards. The positive-pressure PE room is therefore designed to prevent patients from getting exposed to any airborne diseases that may be in the vicinity of the room.
ANSI/ASHRAE/ASHE Standard 170 requires a minimum of 12 air changes of supply airflow per hour and must maintain a minimum 0.01-inch wc positive-pressure differential to the adjacent corridor, whether an anteroom is utilized or not. When an anteroom is provided, airflow should be from the PE room into the anteroom and from the anteroom into the corridor. To maintain the required pressure differential, the supply air quantity must always be higher than the exhaust airflow. Typically, a minimum airflow difference of 20% is usually adequate to maintain pressure differential in a well-sealed room. The final differential airflow will need to be determined by the TAB contractor. In order to ensure these rooms are operating per design ANSI/ASHRAE/ASHE Standard 170, permanently installed visual devices or mechanisms to constantly monitor the air pressure differential should be implemented (when occupied by patients with compromise immune systems).
ANSI/ASHRAE/ASHE Standard 170 recommends supply air diffusers for the PE room should be located in the ceiling above the patient bed, and the return air grille should be located in the ceiling near the door. The supply diffuser shall be a non-aspirating, laminar-flow device designed to limit the air velocity at the patient bed to reduce the possibility of patient discomfort.
Conclusion
Proper air distribution in critical facilities is very important because it contributes positively to the healing environment for patients and enhances the wellness and workplace quality of the staff. Good air distribution is very important for IAQ and the comfort of the patients, staff, and visitors. Poor air distribution is linked to hospital acquired infections because of the role it plays in minimizing the spread of airborne infection. While the quantity of air distributed to the space is important from an air quality standpoint, space pressurization is perhaps even more important for critical spaces in health care settings.
Engineers must be certain air quantities are balanced so that air travels from the cleanest to the dirtiest spaces. They should also ensure the overall building pressure is positive to the outside to prevent the ingress of contaminants into the building. Engineers must design the space to ensure the outside air brought into the health care facility is properly filtered, the air temperature and humidity is within the comfort limits, and the air that is within the space is not allowed to contaminate other patient areas as it is routed back through the return system.
Looking for a reprint of this article?
From high-res PDFs to custom plaques, order your copy today!







