Would ASHRAE 170 Benefit From More Health Data Research?
As we continue to look for weapons to fight hospital-acquired infections (HAI), what does the standard for health care facility ventilation already contain in the way of health metrics? How would a study look if it focused on the one metric that drives so many other decisions in health care? Let’s explore.
FIGURE 1. New opportunity at the intersection of indoor air management, microbiology of the hospital environment, and patient outcomes.
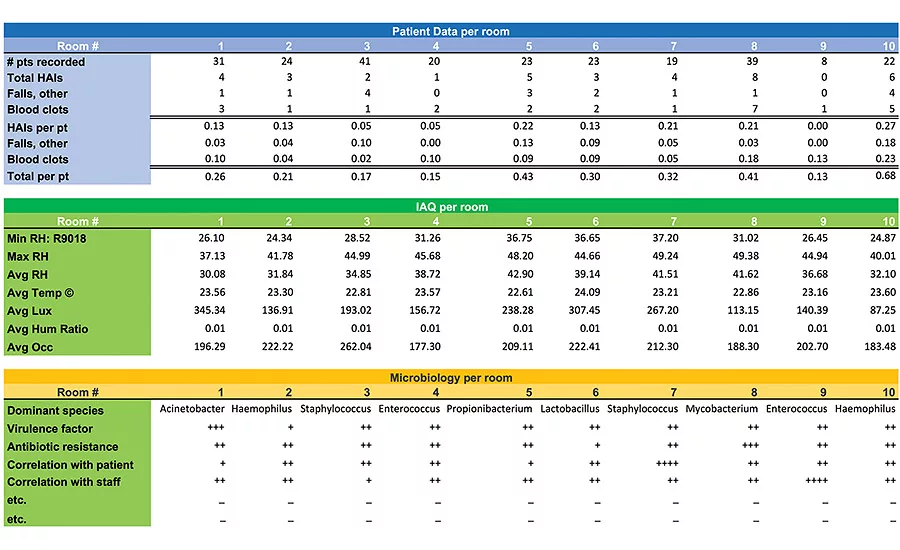
FIGURE 2. Sample data.
As a physician, I say, “Yes.” However, building managers and engineers sometimes answer differently.
One engineer responded to the proposal of physician participation in ASHRAE research as follows:
“We only have certain instrumentalities available to us, primarily having to do with the design, specification, selection, installation, and operation of HVAC equipment. I fear that wide-ranging IAQ research [on occupant health] will suggest complex, esoteric, unproven ‘solutions’ to health issues that will not be helpful and ultimately have little meaning to ASHRAE members”.
Yet, the ASHRAE mission statement says, “To advance the arts and sciences of heating, ventilation, air conditioning, and refrigeration to serve humanity and promote a sustainable world.” In serving humanity, the interaction of IAQ and patient wellbeing is important!
The idea that building science benefits from physician knowledge on occupant health dates back at least as far as Hippocrates’ work in 400 BC. In 1546, Hieronymus Fracastorius published De Contagione, postulating that infectious diseases were spread by “invisible living seeds” which were dispersed by direct contact with infected persons, indirect contact with fomites, and airborne transmission. In the 1850s during the Crimean War, Florence Nightingale revealed the hospital’s contribution to patient deaths with statistical graphics which clearly correlated disease transmission within hospitals with the building water source, air movement, and floor plan design.
In 1975, the United States Center for Disease Control completed a 10-year investigation on patient infections acquired during hospitalization (HAIs). This study revealed the alarmingly high number of HAIs and officially implemented the role of infection prevention in health care facilities. Sadly, 40 years later, largely preventable HAIs affect up to 10% of the patient population and place a large burden on direct hospital costs — and an even higher burden on society as a whole.
What more can be done to protect patients, and how can indoor air management in hospitals help curtail transmission of HAI microbes? Current infection control practices focus on reducing pathogen transmission through behavioral interventions such as monitoring staff hand hygiene, implementing procedure checklists, and emphasizing surface disinfection. These interventions have successfully reduced the detection of many pathogens in the patient environment; however, the correlation with clinical outcome is less clear.
Another approach, called “Evidence-Based Design,” links the spatial design of a hospital with patient outcome in an endeavor to create “healing environments.” While these studies lay a foundation for understanding how the hospital environment affects patient outcomes, we still do not fully understand the role of indoor air management in pathogen transmission and patient infections. As hospitals continue to invest money in strategies to eradicate microbes on surfaces, the role of hospital IAQ in the cycle of HAI transmission is neglected.
This is where ASHRAE standards can be invaluable to hospitals, but we must investigate how closely the existing indoor air recommendations focus on patient health, and ask if there would be benefits from medical expertise.
HEALTH METRICS IN ASHRAE STANDARDS
What human health metrics can already be found in ASHRAE standards? Thermal control guidelines do reference physiology metrics such as surface perspiration and evaporative cooling, core body temperature, circulation, metabolic heat production, etc.
The rationale for controlling fine particulate dissemination is also based on disease metrics such as cancer, dermatitis, asthma, and lung disease using the DALY statistics to define harm.
Correctly, airborne infectious bioaerosols are understood to have additional disease pathways through infection, allergies, and toxicity. The Wells-Riley equation, a standard model of airborne infection, is used to represent dynamics between key variables. This model roughly predicts the number of new infections (C) based on the number of susceptible secondary patients (S), the number of initial infections (I), the number of infectious doses of airborne pathogens (q) expelled into the air per unit time, pulmonary ventilation rate per susceptible secondary patient (p), exposure time (t), and volume flow rate of fresh or disinfected air into which the infectious doses are distributed (Q).
C = S(1 – e–Iqpt/Q)
After exposure, the microorganism must reach the target in the body (e.g., lung or mucosa) to cause infection. While this equation predicts exposure to fungal, bacterial, or viral bioaerosols, it does not predict active infection because several of the variables are rough estimations.
This equation presents an accurate and scientific way to think about airborne transmission. The problem arises with the following statement found in aerobiology literature:
“An organism that does not remain virulent in the airborne state does not cause infection, regardless of how many units of organisms are deposited in the respiratory tract.”
A full discussion of the accuracy of environmental sampling techniques in counting viable bioaerosols is beyond the allowable length for this article. However, in summary, the results are conflicting and contradictory. This makes evaluation of the airborne route of pathogen transmission very difficult, and it impedes the ability to assess different air-cleaning strategies.
Given the limitations of air sampling tests, how can we adequately design and manage HVAC systems to reduce patient harm from HAIs?
We must answer this question:
Which aspects of IAQ improve patient outcomes through decreasing HAIs?
Thankfully, there is an accurate and relevant bio-indicator for assessing the ecological health of the hospital. This bio-marker is the hospitalized patient! The patient, yielding vast amounts of clinical data from body fluid tests, cultures, electronic monitoring, and radiologic imaging, is the ideal “tool” to correlate indoor air management with the microbes that cause HAIs.
By identifying pathogen reservoirs and airborne vectors in the built environment, hospitals can be designed and maintained to improve patient healing, decrease prolonged hospitalizations, and reduce readmissions and mortality. With this information, infection control strategies which currently focus on clinical staff behavior can incorporate new opportunities for reducing HAI rates.
THE MOST IMPORTANT METRIC: PATIENT OUTCOME
A possible study design:
Use the patient as the bio-marker to investigate the health and the role of the built environment and IAQ in infection transmission to identify building components that relate directly to clinical outcome.
Correlate patient pathology with building management to assess factors that both contribute to and decrease patient HAIs.
The results will clearly elucidate optimal building layout, choice of mechanical systems, and air handling parameters, increasing our understanding of the role of the built environment in HAI transmission.
A hypothetical study – Data to collect
Patient data relating to possible HAIs (partial list)
-
Methicillin-resistant Staphylococcus aureus (MRSA) documented after admission
-
Urinary tract infection
-
Wound infection
-
Positive blood culture
-
Positive central line culture
-
Clostridium difficile positive stool
-
Readmission within 30 days of discharge
-
Documented HAI
-
Medications record indicating broad spectrum antibiotic usage
-
Laboratory results
Building spatial and design elements of patient rooms with and without HAIs
-
Single vs. multi-patient room
-
Presence of a room entry vestibule
-
Operable or inoperable windows
-
Inboard or outboard bathroom
-
Room cleaning schedule and protocol
-
Wall, ceiling, floor, and other surface materials in the patient room
-
Placement of family area in room
-
Plants in room
-
Personal protection equipment in use
-
Visitor and clinical staff traffic
Design and maintenance of HVAC systems
-
Air filtration of incoming or outgoing air
-
Type of HVAC system
-
Indoor air relative humidity and temperature
-
Room pressurization and air changes
-
Room air seals
-
Ultraviolet germicidal radiation cleaning in room or ductwork
-
Recirculated or fresh air ventilation
-
Location of air intake and exhaust grills
-
Building or mechanical system maintenance or shutdowns
Use statistical modeling to identify both positive and negative relationships between patient HAIs and the indoor building:
-
Stratify patient rooms according to patient clinical acuity.
-
Control for confounding variables (acuity, age, etc.) through multiple variable regression analysis.
-
Identify correlations between patient HAIs and physical characteristics through data analysis.
Studying patient outcomes to evaluate treatment efficacy is not a new approach in medicine. In the last 15 years most medical and surgical protocols have been rigorously tested in well controlled prospective and double-blind studies. Currently, evidence-based guidelines drive everything from clinical treatment plans to physician reimbursement and health care insurance coverage.
Surprisingly, while HAIs add great cost to health care institutions every year, there are few studies addressing infection control interventions and patient clinical outcome. Hand-hygiene interventions have proven to be successful based on widespread hand cleansing stations and relatively simple implementation, but improved hand hygiene alone has not sufficiently curbed the epidemic of HAIs.
Clinical medicine interventions have greatly benefited from decisionmaking based on statistical analysis of patient outcome. Hospital design and maintenance, an essential component of in-patient treatment, can also improve patient outcome by using these tools. Identification of the optimal HVAC design and management parameters is the next step towards a safer health care setting. This study design using the patient bio-marker will provide essential data needed to take patient safety to new heights.
Looking for a reprint of this article?
From high-res PDFs to custom plaques, order your copy today!




